
At the recently convened Malaysian Economic Forum, Health Minister Dr Dzulkefly Ahmad outlined the main features of the Ministry of Health’s plan to “reset” the Malaysian healthcare system.
At first glance, the new strategy might appear comprehensive and reasonable. It attempts to tackle some of the major problems plaguing our public health services.
However, it does not adequately address some crucial issues. But first, a quick look at what the ‘reset’ plan actually involves.
The five-point plan
The Rakan KKM (Friends of the MoH) scheme is a key component of the reset.
It involves setting up special clinics within government hospitals, where paying patients can cut the queue and see the specialist of their choice. Where needed, that specialist will conduct whatever procedures are required – for a fee, probably around 70–80% of what private hospitals charge.
- Sign up for Aliran's free daily email updates or weekly newsletters or both
- Make a one-off donation to Persatuan Aliran Kesedaran Negara (ALIRAN), Maybank a/c 507246118995 or CIMB a/c 8004240948
- Make a pledge or schedule an auto donation to Aliran every month or every quarter
- Become an Aliran member
The rationale is threefold.
First, the extra income government specialists earn from these clinics is intended to induce them to stay in government service.
Second, the money the government collects from these paying patients – for investigations, use of operating theatres, medications and so on – will augment MoH funds.
Third, the lower prices at Rakan KKM clinics are meant to act as a brake on private hospital charges. Private hospitals, the thinking goes, will be constrained from raising their fees too high if patients have the option of going to Rakan KKM instead. The inflation in healthcare costs in Malaysia will thus be controlled to an extent.
A dedicated national health fund will be set up to receive income from the Rakan KKM clinics.
Rather than being channelled to the Consolidated Fund as currently happens with all fees collected by government hospitals and clinics, this money will instead be placed in the new fund and used to upgrade the public healthcare system.
The MoH’s allocation in the 2026 Budget is RM46.5bn – the second-highest among all ministries, yet still insufficient for all the repairs, procurement and upgrading required. (Dzulkefly has acknowledged feeling constrained from requesting a higher allocation, given that Malaysia’s estimated fiscal deficit for 2026 stands at about RM76bn or 3.5% of GDP, and the federal government’s total debt is now approaching RM1.3tn or 64% of GDP.)
The extra income from Rakan KKM is meant to make up some of the shortfall.
The third component is the Base MHIT (medical and health insurance or takaful), a no-frills health insurance policy to be set up by the government. It would include features such as co-payments and annual caps (reportedly around RM100,000 per year) to encourage patients to use the facility judiciously and keep costs down.
The co-payment element appears deliberate: when patients face no out-of-pocket costs at all, they have less incentive to question their healthcare provider about different investigation and treatment options, which leads to over-investigation, escalating costs and, ultimately, rising insurance premiums.
In addition to offering more affordable insurance options, the Base MHIT would also help moderate inflation in private health insurance premiums, since patients would have the option of switching to the government scheme.
Electronic medical records form the fourth component. All investigations and treatment carried out in both the public and private sectors would be loaded onto a patient’s electronic medical records, cutting costs and time by reducing duplication of investigations.
Finally, the government will introduce a diagnosis-related group system for billing by the private sector. Private hospitals would only be allowed to charge a fixed amount for each DRG – a measure aimed at reducing overcharging.
Where the plan falls short
The socialist party PSM has serious concerns about several aspects of this ‘reset’ strategy. Dzulkefly has accused us of misrepresenting facts and playing politics. But our reasons are valid, as set out below.
The specialist shortage problem: At present, only 25% of specialists with more than five years’ post-specialisation experience are in the public sector. Yet 75% of in-patients are treated in public hospitals.
There is therefore a large mismatch of resources, and patients in government hospitals already endure long waiting times to see a specialist.
The Rakan KKM is good for the top 20% of households and the upper-middle class, who can afford private care or who now have an additional option if private hospitals become too expensive.
But it comes at the expense of the 75% of patients who depend on the public healthcare system. Their access to government specialists will be further impaired and their waiting times will increase further.
This is why we are calling for the Rakan KKM scheme to be cancelled. It will marginalise the bottom 70% of the population.
The salary gap is too wide to bridge: We do not believe the extra RM3,000 to RM6,000 that government specialists can earn through Rakan KKM can counter the predatory recruiting practices of private hospitals.
When one private hospital group opened a new hospital in Ipoh last year, 16 specialists from public hospitals – including 12 from Ipoh General Hospital – resigned from government service to join the new hospital.
Some of those specialists told us they had been guaranteed a monthly income of RM70,000 for the first year, with Sunway topping up their earnings if their patient load did not reach that target.
Among those who left were two anaesthetists, a cardiologist, a dermatologist, an emergency medicine specialist, an ENT specialist, a gastroenterologist, a general surgeon, a geriatrician, a neurosurgeon, an oncologist, two paediatricians, a radiologist, a respiratory physician and a urologist.
How can an additional RM6,000 a month through Rakan KKM neutralise that kind of pull factor?
Our proposal is a five-year moratorium on new private hospitals. This would cost the government nothing extra and would not adversely affect specialists already in private practice.
We are also calling on the government to establish a separate service commission for the public healthcare sector – something the Malaysian Medical Association (MMA) has been requesting for decades.
A separate commission would make it possible to offer better remuneration for healthcare staff, perhaps modelled on the pay structure at IJN, the national heart institute.
Low wages mean low insurance coverage: Malaysia has pursued a low-wage policy for decades as part of its strategy to attract foreign direct investment.
As a result, the median wage in the formal sector stands at around RM3,000 per month.
Only around 22% of households currently have health insurance. These are the people who might benefit from Rakan KKM and the Base MHIT.
We have no objection to any programme that benefits the upper-middle class – provided it does not marginalise the bottom 75%.
The inescapable fact is that Rakan KKM will make specialist care even less accessible to the B40 and most of the M40. That is why we are asking for it to be abandoned.
The deeper problem: chronic underfunding
Malaysia has chronically underfunded its public healthcare system for decades.
According to World Health Organization (WHO) data:
Even Thailand puts a larger share of its GDP into public healthcare. If Malaysia genuinely aspires to be a high-income nation, shouldn’t we benchmark ourselves against Britain, Japan and Germany – countries that allocate 9–10% of GDP to public healthcare?
This is the basis for our proposal that the healthcare budget should be increased to 5% of GDP over the next five years.
We are not a poor country. Our GDP grew from RM11.8bn in 1970 to RM1.5tn in 2019 – a nominal increase of roughly 127 times. Once you adjust for inflation, with the Consumer Price Index rising about 5.1 times over the same period, real GDP still grew 25-fold in under 50 years.
So how is it that we cannot find the funds to look after the health of our people?
The answer lies in the gross maldistribution of national income.
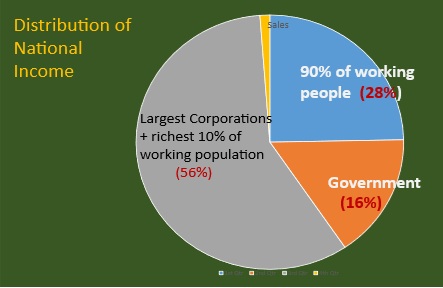
Of Malaysia’s national income of roughly RM2tn per year, an estimated 56% accrues to the top 10% of the population and the largest companies. The bottom 90% receive around 28%, while the government receives only 16%.
Our proposal is that the share going to the largest companies and the top 10% could be reduced by five percentage points, channelling an additional 5% of GDP into government revenue. That would put an extra RM100bn into the federal budget.
We want the “Madani” (compassionate) government to seriously consider the following questions.
Why has government revenue dropped from around 30% of GDP in the 1980s to only 16% of GDP today?
Why have corporate taxes fallen from 40% of profits in the 1980s to the current rate of 24%?
Is the race among Asean nations for foreign direct investment the cause of this decline in corporate taxes? If so, why hasn’t the Malaysian government initiated talks with Asean neighbours about halting this race to the bottom?
What needs to change
These are reasonable questions to put to our government.
We hope that people across Malaysia will raise them with their MPs –particularly as the general election draws closer. Ask your MPs to push for the cancellation of the Rakan KKM scheme, a five-year moratorium on new private hospitals, a separate health commission to ensure better salaries for public-sector health staff, and an increase in the MoH budget allocation to 5% of GDP.
To be clear, we do not object to the Base MHIT, electronic medical records or the diagnosis-related group system for private hospital charges – provided the Rakan KKM scheme is cancelled. All these initiatives, if properly conceived and implemented, can improve healthcare in Malaysia.
Our objection is specifically to the elements of the ‘reset’ that will make things worse for those who can least afford it.
If enough people raise these issues, the government will have to listen.
A nation’s healthcare system says a great deal about the values of that nation – how compassionate we are towards the sick, older people and the poor; whether we are building a system based on solidarity that ensures everyone receives the healthcare they need, regardless of social or economic status; and whether we are doing enough to support healthcare personnel in the public sector who are already working impossibly long hours.
What is at stake here is not just healthcare, but the soul of the nation. We hope you will join us in safeguarding and rehabilitating our healthcare system. We owe that to ourselves, our children and our country.
AGENDA RAKYAT - Lima perkara utama
- Tegakkan maruah serta kualiti kehidupan rakyat
- Galakkan pembangunan saksama, lestari serta tangani krisis alam sekitar
- Raikan kerencaman dan keterangkuman
- Selamatkan demokrasi dan angkatkan keluhuran undang-undang
- Lawan rasuah dan kronisme
